









Contents
- Endometriosis, what is it?
- Who are the “at risk” people?
- How to recognize the first signs of endometriosis?
- How to diagnose endometriosis?
- What are the possible complications of endometriosis?
- Endometriosis: what is the current treatment?
- In video: Diet, which foods to favor and which to avoid to reduce the symptoms associated with endometriosis? Catherine Malpas, naturopath, answers us.
- Is pregnancy possible despite endometriosis?
Endometriosis, what is it?
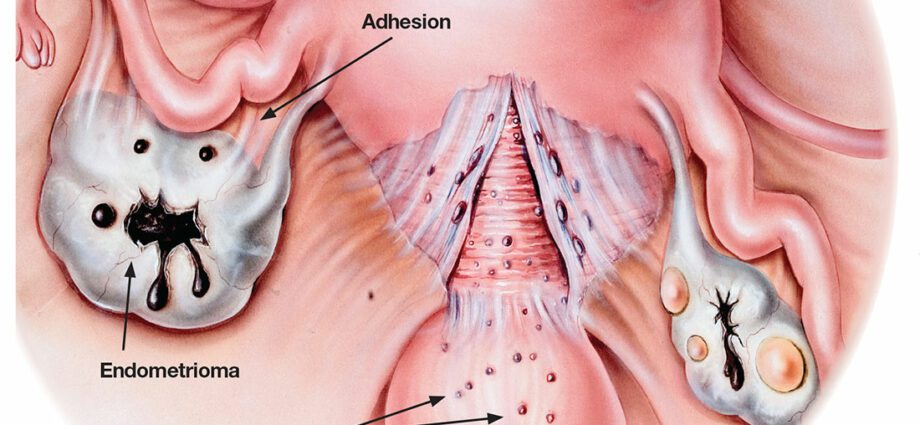
The endometrium is a lining of the uterus. Under the effect of hormones (estrogen and progesterone), during the cycle, the endometrium thickens at the time of ovulation, and if there is no fertilization, it breaks down and bleeds. These are the rules. Endometriosis is a disease caused by tissue similar to endometrial tissue that migrates and grows outside the uterus, then causes lesions, adhesions and cysts in colonized organs. In some cases, the lesions can infiltrate deep into the walls of the pelvic organs over time (digestive system, bladder, etc.). This is called deep endometriosis which is one of the most severe forms of the disease. In contrast, we call superficial endometriosis an endometriosis that affects only the tissues surrounding the uterus (tubes, ovaries). Since these are pieces of the endometrium, the endometriosis lesions will behave each month like the endometrium: they will thicken under the effect of hormones and bleed, causing pain during periods and / or sexual intercourse, or when going to the bathroom, depending on the location of the lesions.
Note: to date, there are only theories on the origin of this disease which remains a “mystery” for doctors. Genetic (familial forms) and environmental (pollution, endocrine disruptors, hormones) factors have been put forward.
Who are the “at risk” people?
The average age of discovery of the disease is around 27 years old but, all women can be affected by this disease, as long as it is regulated. Often these are young women without children. However, it also happens that endometriosis appears after pregnancy. Note that women with endometriosis have generally had very severe pain during their period, sometimes preventing them from going to school or work. The existence of difficult periods in the adolescent could, in fact, constitute a precursor state of the disease. In addition, it is common to find relatives suffering from this pathology in the first degree.
In recent years, this disease has been mentioned openly. There are more and more associations of sick women,
How to recognize the first signs of endometriosis?
Distinguishing between “normal” period pain and “abnormal” pain is very difficult, not only for women, but also for doctors. The women concerned are those who have recurrent pain during menstruation, requiring medical treatment (eg Antadys). These same women sometimes cannot get up in the morning because they are in so much pain or have to be on sick leave. You should know that the pain can increase over time and not be limited only to the period of the rules. Painful intercourse, genes during defecation or urination at the same time as menstruation, can also be thought of as endometriosis. But it also happens that the disease does not manifest itself with these symptoms, it can be “silent”. The diagnosis of endometriosis is then most often made when the woman consults because she is unable to have a baby.
How to diagnose endometriosis?
The disease is often diagnosed during an infertility workup prescribed to couples having difficulty conceiving. Pelvic pain can also alert doctors who then order an ultrasound, sometimes an MRI. Finally, it is sometimes the discovery of a cyst on a routine ultrasound that is the revealing element.
Un clinical examination (interrogation, vaginal examination) conducted by a specialist in this disease often gives a relatively precise idea of the extent of the lesions. MRI or ultrasound, when done by doctors who have experience with this condition, can also provide answers. However, the diagnosis with certainty is difficult to obtain, because the only way to fully know the severity of the lesions is to perform a laparoscopy. During this surgical intervention, the surgeon takes a sample of the lesions in order to analyze them and establish the diagnosis.
Endometriosis is a fairly complex disease that is difficult to diagnose. The time to diagnosis is approximately seven years, which is considerable. Patients and doctors each have a share of responsibility. On the one hand, women are slow to go for a consultation because their painful periods are part of their life and they think that it is “normal to be in pain” as their own mother and grandmother told them before. On the other side, doctors often underestimate women’s complaints, and prescribe pain relievers or pills that mask symptoms without even having been diagnosed with the disease. It is important that the subject of endometriosis is studied in depth during the studies of future doctors, but also of midwives in order to reduce this diagnostic time.
What are the possible complications of endometriosis?
The main risk associated with endometriosis is infertility. About 30-40% of women with endometriosis will experience infertility. And one in 3 women who have trouble getting pregnant has endometriosis. The many adhesions can damage the tubes and ovaries (even block them), and make the uterus inhospitable. The doctor may suggest a medical or surgical strategy, depending on the diagnosis. The first-line approach is to take a continuous pill to block menstruation, and thus slow down the progression of the disease. Surgery aims to remove as many lesions as possible, with the aim of reducing pain and / or increasing the chances of pregnancy.
Note: it is better not to delay a desired pregnancy too much, because the more time advances, the more the chances of conceiving naturally diminish.
Endometriosis: what is the current treatment?
Management varies from patient to patient because endometriosis manifests itself differently in each person. If a woman’s priority is to treat her pain, we often start by prescribing a pill continuously. The goal is to achieve amenorrhea (menstruation suppression) with blockage of ovulation and decrease in estrogen levels. Putting the ovaries at rest by making the cycles disappear helps reduce pain, although this does not permanently resolve endometriosis. Another option is possible: analogues of Gn-RH. These are drugs that put the patient in a state of artificial menopause. However, they can have serious side effects, such as hot flashes, decreased libido or osteoporosis. Their prescription should not go beyond one year. When pain resists medical treatment, surgery is the alternative. Laparoscopy with removal of all endometriotic lesions is the technique of choice, subject to a favorable risk / benefit balance for the patient.
Food, how can it help us reduce the symptoms of endometriosis?
In video: Diet, which foods to favor and which to avoid to reduce the symptoms associated with endometriosis? Catherine Malpas, naturopath, answers us.
Is pregnancy possible despite endometriosis?
About 30-40% of affected women have difficulty getting pregnant. Endometriosis is a cause of infertility, but not the only one. The existence of endometriosis, the age of the woman, her ovarian reserve, the permeability of the tubes are all the elements to be taken into account in deciding the best strategy. We have two options: surgery and medically assisted procreation (MAP). Studies show that the results in terms of fertility are significantly increased when the surgical removal of the lesions is complete. However, it is still possible to opt for ART without having previously performed surgery. Depending on the severity of the endometriosis, there are several treatment options: ovarian stimulation with intrauterine insemination and IVF.