









Contents
Pompe disease
What is it ?
Pompe disease is the name commonly given to “type II glycogenosis (GSD II)”.
This pathology is characterized by an abnormal accumulation of glycogen in the tissues.
This glycogen is a polymer of glucose. It is a carbohydrate formed from long chains of glucose molecules, forming the main store of glucose in the body and thus constituting an important source of energy for humans.
Different forms of the disease exist depending on the symptoms and the chemical molecules found in the tissues. Certain enzymes are thought to be responsible for this abnormal accumulation of glycogen. These include the glucose 6-phosphatase, In theamylo-(1-6)-glucosidase but above all fromα-1-4-glucosidase. (1)
This is because the latter enzyme is found in an acidic form in the body and is capable of hydrolyzing (destroying a chemical by water) glycogen into units of glucose. This molecular activity therefore leads to an intralysosomal (intracellular organelle in eukaryotic organisms) accumulation of glycogen.
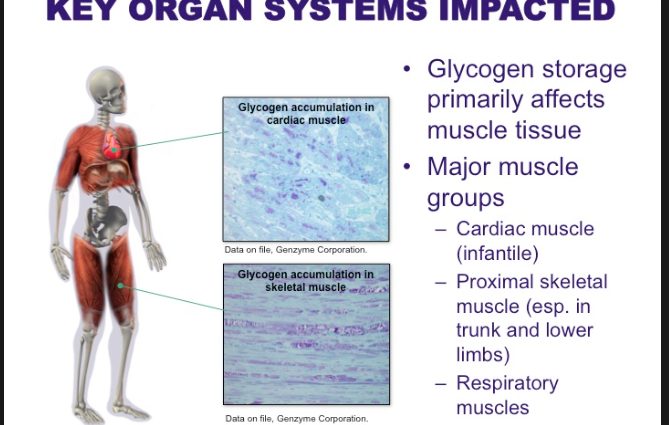
This α-1,4-glucosidase deficiency is expressed only by certain organs, and especially the heart and skeletal muscle. (2)
Pompe disease results in skeletal and respiratory muscle damage. Hypertrophic heart disease (thickening of the heart structure) is often associated with it.
This disease affects adults more. However, the symptoms associated with the adult form differ from the symptoms associated with the infantile form. (2)
It is an inherited pathology by autosomal recessive transmission.
The gene encoding the α-1,4-glucosidase enzyme is carried by an autosome (non-sexual chromosome) and the recessive subject must have two identical alleles in order to express the phenotypic characteristics of the disease.
Symptoms
Pompe disease is therefore characterized by an accumulation of glycogen in the lysosomes of the skeletal muscles and the heart. However, this pathology can also affect other regions of the body: the liver, the brain or the spinal cord.
The symptoms are also different depending on the affected subject.
– The form affecting the newborn is mainly characterized by hypertrophic heart disease. It is a heart attack with thickening of the muscle structure.
– The infantile form generally appears between 3 and 24 months. This form is defined in particular by respiratory disorders or even respiratory failure.
– The adult form, for its part, is expressed by progressive cardiac involvement. (3)
The main symptoms of type II glycogenosis are:
– muscular exhaustion in the form of muscular dystrophies (weakness and degeneration of the fibers of the muscles which lose their volume) or myopathies (set of diseases affecting the muscles), which results in chronic fatigue, pain and weakness muscle. The muscles affected by this disease are both locomotor, respiratory and cardiac muscles.
– an inability for the organism to degrade the glycogen accumulated in the lysosome. (4)
The origins of the disease
Pompe disease is an inherited disease. The transfer of this pathology is autosomal recessive. It is therefore the transmission of a mutated gene (GAA), located on an autosome (non-sexual chromosome) located on chromosome 17q23. In addition, the recessive subject must contain the mutated gene in duplicate to develop a phenotype relating to this disease. (2)
Hereditary transmission of this mutated gene results in a deficiency of the enzyme α-1,4-glucosidase. This glucosidase is deficient, so glycogen cannot be degraded and then accumulates in the tissues.
Risk factors
The risk factors for developing Pompe disease lie exclusively in the parental genotype. Indeed, the origin of this pathology being autosomal recessive inheritance, it requires that both parents carry the mutated gene encoding an enzymatic deficiency and that each of these genes are found in the cells of the newborn so that the disease breaks out.
The pre-natal diagnosis is therefore interesting to know the possible risks that the child develops such a disease.
Prevention and treatment
The diagnosis of Pompe Disease should be made as soon as possible.
The early infantile form is quickly detectable through significant cardiac muscle enlargement. The diagnosis of this form of the disease must therefore be made urgently and treatment must be put in place as soon as possible. Indeed, in this context, the vital prognosis of the child is rapidly engaged.
For the “late” form of childhood and adults, patients risk becoming dependent (wheelchair, respiratory assistance, etc.) in the absence of treatment. (4)
Diagnosis is mainly based on a blood test and a specific genetic test for the disease.
Biological screening consists of the demonstration of an enzymatic deficit.
A pre-natal diagnosis is also possible. It is a measure of the enzymatic activity within the framework of a trophoblast biopsy (cell layer made up of fibroblasts giving rise to the placenta in the third month of pregnancy). Or by identifying specific mutations in fetal cells in the affected subject. (2)
Enzyme replacement therapy may be prescribed for a subject with Pompe disease. This is alglucosidase-α. This recombinant enzyme treatment is effective for the early form but has not, however, been proven to be of benefit in the later onset forms. (2)